A headache is one of the most common complaints I hear in clinic, and the vast majority have nothing to do with a brain tumour. But a small proportion of patients who come to me with persistent or unusual headaches do have one, and in those cases, recognising the warning signs early genuinely changes the outcome. As a Consultant Neurosurgeon at DRM Multispeciality Hospital, Mysore, with 13 years of experience and more than 6,000 complex brain and spine surgeries, I want to give patients and families a clear, honest framework for understanding which symptoms warrant urgent evaluation and which almost certainly do not. This is not designed to cause alarm. It is designed to replace uncertainty with clarity about brain tumour symptoms.
Why brain tumour symptoms are so often confused with other conditions
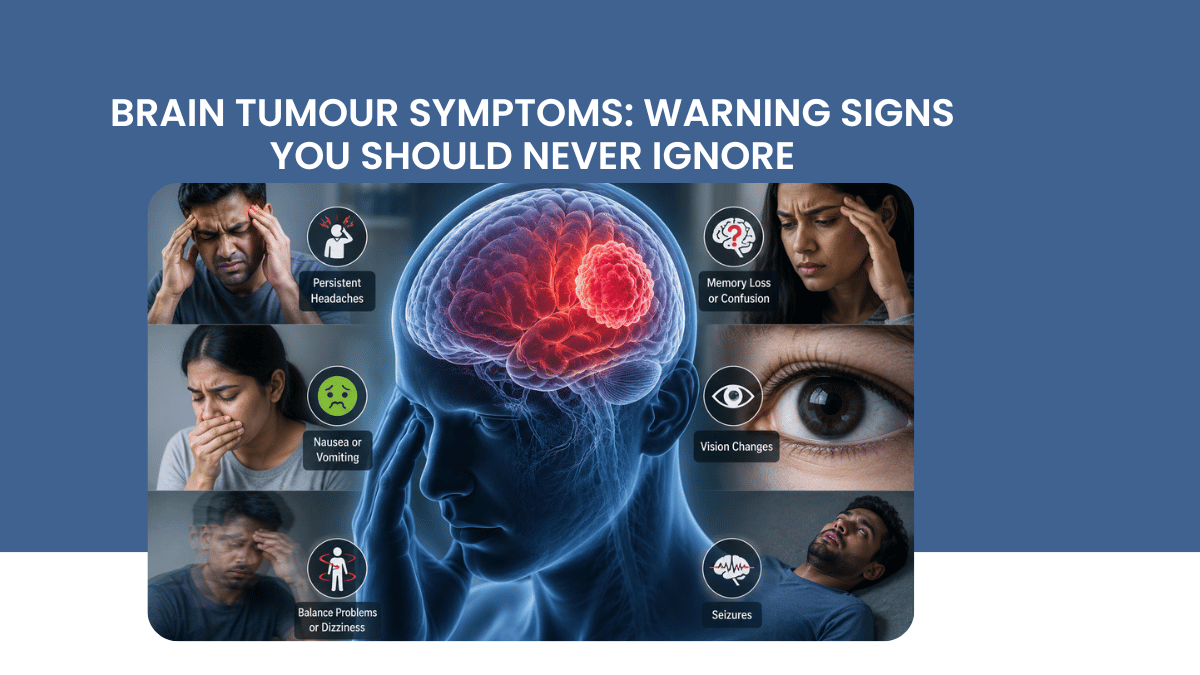
The brain controls everything: movement, sensation, vision, speech, memory, mood, and coordination. This means that a growing mass inside the skull can produce an enormous range of symptoms depending entirely on its location, its size, and how quickly it is growing. A tumour in the frontal lobe might cause personality change long before it causes a headache. A tumour near the brainstem might cause balance problems before anything else. This variability is exactly why warning signs of a brain tumour are so frequently mistaken for migraine, stress, vitamin deficiency, anxiety, or simple ageing. Understanding the pattern of symptoms, not any single symptom in isolation, is what actually helps distinguish a tumour from something far more common and benign.
Headaches: when they are and are not a warning sign
Most headaches are not caused by a brain tumour. Tension headaches and migraines are vastly more common and have well-recognised patterns. What distinguishes a headache caused by brain tumour from an ordinary headache is the pattern, not the intensity alone. A headache that is new in a person who has never had significant headaches before, that is progressively worsening over weeks rather than staying stable, that is worse in the morning and improves through the day, that wakes a person from sleep, or that is worsened by coughing, straining, or bending forward, deserves evaluation. So does a headache accompanied by vomiting that is not explained by another illness, particularly vomiting without nausea, which can be a specific sign of raised pressure inside the skull.
A single bad headache, even a severe one, in someone with a known history of migraine is rarely cause for alarm on its own. It is the change in pattern, the persistence, and the company it keeps with other symptoms that matters most.
Seizures: a first seizure in an adult always needs investigation
A first seizure in an adult who has never had one before is one of the most important presenting symptoms of a brain tumour and should always prompt urgent neurological evaluation, including brain imaging. This applies even if the seizure was brief, even if the person recovered completely afterwards, and even if there is no other symptom present. Children and young adults more commonly have epilepsy unrelated to a tumour, but a new-onset seizure in an adult, particularly someone over 40 with no prior history, carries a meaningfully higher likelihood of an underlying structural cause that needs to be identified or excluded.
Vision changes that should prompt evaluation
Several types of visual disturbance can indicate a brain tumour, particularly tumours located near the optic pathways or pituitary gland. Progressive blurring or loss of vision in one or both eyes that is not explained by a refractive error, double vision, particularly if it is new and persistent, loss of peripheral vision noticed when bumping into objects on one side, or visual disturbances accompanied by headache all warrant assessment. Vision changes from brain tumour often develop gradually, which is part of why they are sometimes dismissed as simple ageing of the eyes rather than investigated properly.
Cognitive, personality, and behavioural changes
This is one of the most difficult categories of symptom for families to recognise, because the changes are gradual and the person experiencing them often has reduced insight into the change. A previously organised person becoming forgetful or confused, a usually calm person becoming irritable or impulsive, difficulty with concentration or decision-making that represents a clear change from baseline, or unusual apathy and withdrawal can all reflect a frontal or temporal lobe tumour. Families frequently describe noticing the person is simply not themselves, sometimes months before any other symptom appears. This observation, vague as it may sound, is clinically meaningful and should be taken seriously.
Weakness, numbness, and coordination problems
New weakness or numbness affecting one side of the body, problems with balance and coordination, particularly if they have developed gradually rather than suddenly, and difficulty with fine motor tasks such as buttoning a shirt or writing can all indicate a tumour affecting the motor or sensory pathways or the cerebellum. The gradual nature of onset is an important distinguishing feature: a sudden onset of these symptoms is more typical of a stroke and is a medical emergency requiring immediate attention, while a gradual neurological symptom progression over weeks to months is more typical of a slowly growing tumour, though it still requires prompt evaluation.
Speech and language difficulties
Difficulty finding words, slurred speech, or trouble understanding language can indicate a tumour affecting the language areas of the brain, typically located in the dominant hemisphere. These symptoms are sometimes mistaken for a minor stroke or transient ischaemic attack, particularly when they appear suddenly, and any sudden speech disturbance should be treated as a medical emergency regardless of the eventual cause. A gradual speech difficulty brain tumour that gets progressively worse over time follows a different pattern and warrants neurological assessment with imaging.
Hormonal and endocrine symptoms
Tumours affecting the pituitary gland, located at the base of the brain, can produce symptoms that are easily mistaken for unrelated hormonal or metabolic conditions. These include unexplained weight changes, menstrual irregularities, changes in libido, excessive thirst and urination, unusual growth of hands and feet in adults, or changes in breast tissue or milk production unrelated to pregnancy or breastfeeding. Because these symptoms span endocrinology, gynaecology, and general medicine, pituitary tumour symptoms are sometimes investigated for years through other specialties before a brain tumour is identified as the underlying cause.
When symptoms appear together: why the combination matters
No single symptom on this list, taken in isolation, should cause panic. Headaches, fatigue, and forgetfulness are extremely common and have many benign explanations. What increases clinical concern is the combination and progression of symptoms: a headache that is new and worsening, combined with morning vomiting and a recent personality change, is a very different clinical picture from an isolated tension headache that has been present, unchanged, for years. As a clinician, I weigh the entire pattern, the trajectory over time, and the specific combination of symptoms, rather than reacting to any single complaint in isolation. This is the framework I would encourage every patient and family to use when deciding whether to seek a neurosurgery consultation for a concerning symptom.
How brain tumours are diagnosed
Clinical assessment
The diagnostic process begins with a detailed history, focusing on the onset, duration, progression, and pattern of symptoms, followed by a thorough neurological examination assessing vision, coordination, reflexes, strength, sensation, and cognitive function. This clinical assessment guides which investigations are most appropriate and helps localise which part of the brain may be involved before any imaging is performed.
MRI brain
MRI with contrast is the definitive imaging investigation for evaluating a suspected brain tumour. It provides detailed information about the tumour's location, size, characteristics, and relationship to critical structures, information that is essential for surgical planning. MRI brain tumour diagnosis typically also includes specific sequences to assess blood supply and tumour behaviour, which help predict whether a lesion is likely to be benign or malignant before any biopsy is performed.
Additional investigations
Depending on the location and suspected nature of the tumour, additional investigations may include CT scan, particularly useful for assessing bone involvement near the skull base, blood tests including hormonal panels for suspected pituitary tumours, and in selected cases, a biopsy to confirm tissue diagnosis before definitive treatment is planned. A multidisciplinary discussion involving neurosurgery, neuro-oncology, radiology, and pathology is standard practice for complex cases to ensure the treatment plan reflects the full clinical picture.
What happens after a brain tumour is diagnosed
A confirmed or suspected brain tumour diagnosis does not automatically mean immediate major surgery. Treatment depends entirely on the tumour type, its location, its growth rate, and the patient's overall condition. Some slow-growing, asymptomatic tumours are monitored with periodic imaging rather than treated immediately. Others require prompt surgical intervention, sometimes combined with radiation or chemotherapy depending on the tumour type. The goal of modern brain tumour surgery is not simply maximal tumour removal at any cost, but maximal safe removal that preserves neurological function and quality of life. Advances in microsurgical technique, intraoperative monitoring, and image guidance have significantly improved the safety profile of brain tumour surgery over the past two decades.
Questions patients ask me most often
If I have a headache, does that mean I have a brain tumour?
Almost certainly not. The overwhelming majority of headaches, including severe ones, are not caused by brain tumours. What matters is whether the headache represents a new and progressively worsening pattern, particularly when combined with other symptoms such as morning vomiting, vision changes, or seizures.
Can brain tumours be detected on a routine health check-up?
Not typically, unless the check-up specifically includes brain imaging, which is not part of standard routine screening. Brain tumours are usually identified when a patient presents with a specific neurological symptom and is investigated accordingly. There is currently no recommended brain tumour screening for asymptomatic individuals in the general population, which is precisely why recognising symptoms and seeking timely evaluation matters.
Are all brain tumours cancerous?
No. Many brain tumours are benign, meaning they do not invade surrounding tissue or spread to other parts of the body, though they can still cause significant symptoms by pressing on surrounding brain structures simply due to their location within the confined space of the skull. The distinction between benign and malignant, along with the tumour's specific type, is determined through imaging characteristics and, when needed, tissue diagnosis, and this distinction significantly influences both treatment approach and prognosis.
How quickly should I see a neurosurgeon if I am concerned?
If you are experiencing a new, severe, or rapidly worsening headache with vomiting, a first seizure, sudden weakness, sudden vision loss, or sudden difficulty with speech, seek emergency care immediately. For gradual or persistent symptoms that concern you but are not acute emergencies, a neurosurgical consultation within days to a couple of weeks is appropriate, since most brain tumours grow over months, not hours, and a short delay for proper evaluation rarely changes the outcome.
If you or a family member are experiencing persistent headaches, a first seizure, unexplained vision changes, or any of the symptoms described above, timely evaluation provides clarity and, where needed, the earliest possible access to treatment. To book a consultation with Dr Goutham Cugati at DRM Multispeciality Hospital, Mysore.
Written by Dr Goutham Cugati, MBBS, DNB (Neurosurgery), PGDCR, PGDMLS, Fellowship in Micro-Neurosurgery, Consultant Neurosurgeon and Spine Surgeon, Director, Department of Neurosciences, DRM Multispeciality Hospital, Mysuru, Karnataka.
Add a Comment