A slipped disc, more accurately called a disc prolapse or herniated disc, is one of the most common reasons patients come to see me at DRM Multispeciality Hospital, Mysore, and also one of the most misunderstood. Many patients arrive convinced that a slipped disc automatically means surgery. In reality, the large majority of cases improve with conservative treatment, and slipped disc surgery is reserved for a specific subset of patients where it offers genuine, well-defined benefit.
What actually happens in a slipped disc
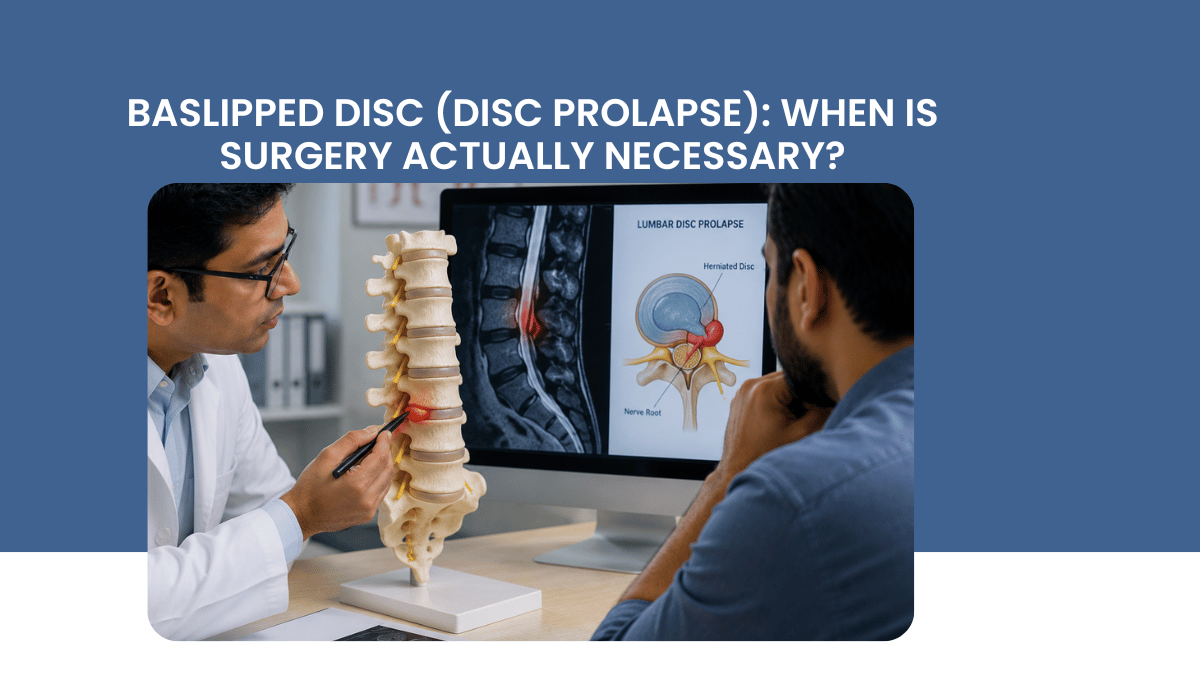
The spine is cushioned between each vertebra by a disc with a tough outer ring and a soft, gel-like centre. A disc prolapse occurs when this outer ring weakens or tears, allowing the inner material to bulge or extrude outward. When this protrusion presses on a nearby nerve root or the spinal cord, it produces the classic symptoms of pain radiating down an arm or leg, numbness, tingling, or weakness, depending on the level of the spine involved and which nerve is affected.
Why most slipped discs do not need surgery
The majority of disc prolapses, particularly those without significant neurological deficit, improve substantially within six to twelve weeks with conservative management. This includes physiotherapy, anti-inflammatory medication, activity modification rather than complete bed rest, and in selected cases, image-guided epidural steroid injections to reduce inflammation around the affected nerve. The body has a genuine capacity to reabsorb extruded disc material over time, and a significant proportion of patients who begin treatment convinced they need surgery find that conservative treatment for disc prolapse resolves their symptoms entirely.
When surgery genuinely becomes necessary
Surgery is appropriate in a specific and well-defined set of circumstances:
- Progressive or significant neurological weakness, such as foot drop or weakening grip, rather than pain alone
- Cauda equina syndrome, a surgical emergency involving loss of bladder or bowel control, saddle numbness, or progressive bilateral leg weakness
- Severe pain that has not responded to six to twelve weeks of appropriate conservative treatment
- Significant, confirmed nerve compression on MRI that correlates directly with the patient's symptoms
Outside of cauda equina syndrome, which requires emergency surgery, the decision to operate is rarely urgent, and there is generally time for a proper trial of conservative management before considering a surgical opinion.
What modern disc surgery actually involves
When surgery is genuinely indicated, the approach has changed significantly over the past two decades. Minimally invasive spine surgery and endoscopic discectomy now allow removal of the herniated disc material through small incisions, using a microscope or endoscope for precision, with significantly less tissue disruption than traditional open surgery. Most patients undergoing minimally invasive discectomy go home within a day or two and return to light activity considerably faster than with older surgical techniques.
If you have persistent back or leg pain, numbness, or weakness that has not improved with appropriate conservative treatment, a spine evaluation will clarify whether surgery is genuinely indicated or whether continued conservative management is the right path. To book a consultation with Dr Goutham Cugati at DRM Multi-Speciality Hospital, Mysore.
Written by Dr Goutham Cugati, MBBS, DNB (Neurosurgery), PGDCR, PGDMLS, Consultant Neurosurgeon and Spine Surgeon, Director, Department of Neurosciences, DRM Multispeciality Hospital, Mysuru, Karnataka.
Add a Comment