Many regions screen infants for congenital adrenal hyperplasia (CAH) due to 21‑hydroxylase deficiency and congenital hypothyroidism —a serious but treatable disease if detected early.



Dr. Anjana Hulse
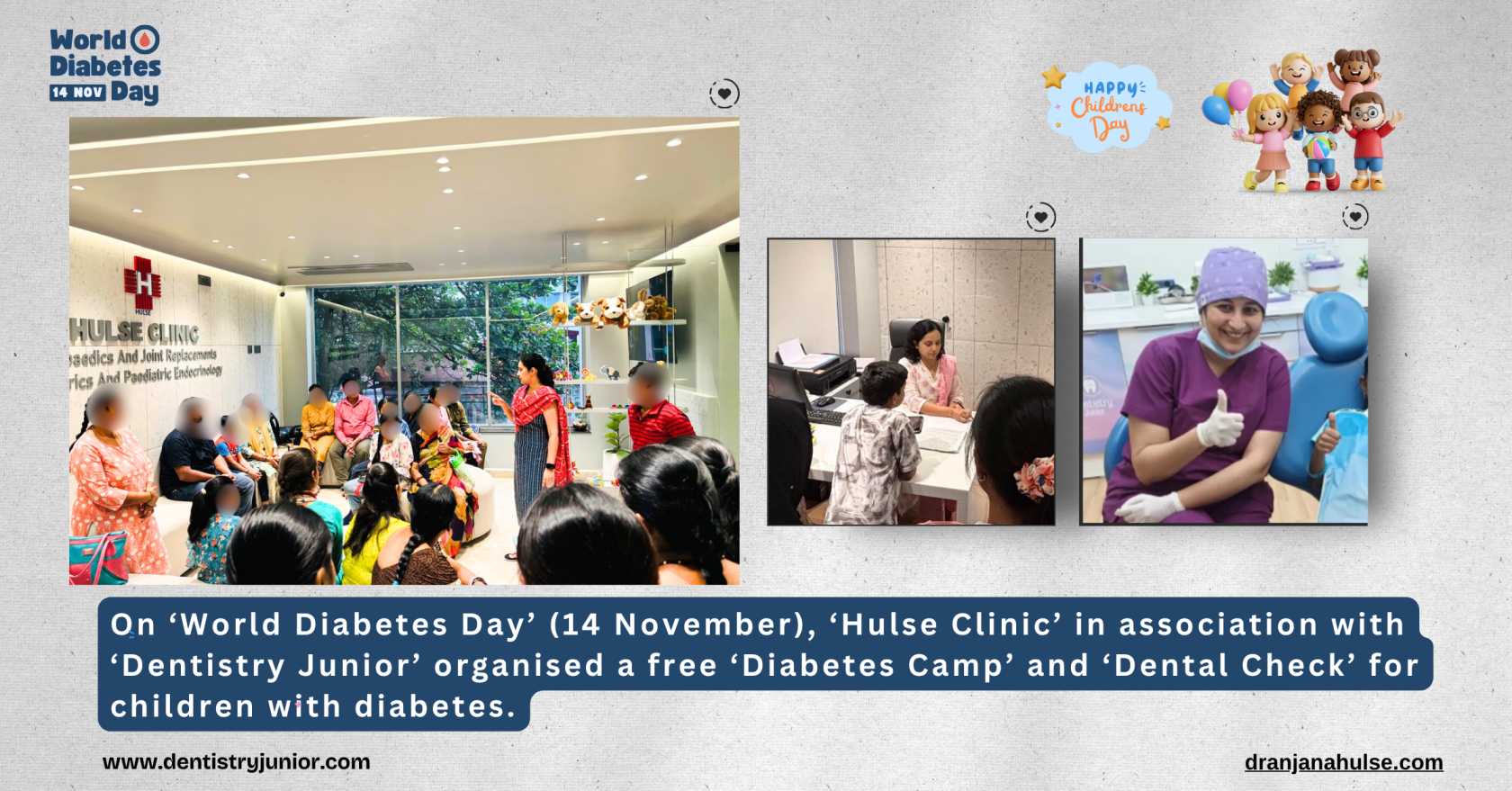
Nurturing Young Lives: Expert Care for Paediatrics and Paediatric Endocrinology
MBBS, MRCPCH, MSc (Paed Sc. - Endrocrinology) (UK)

20 Years of Experience
25000+ Patients
About Dr. Anjana Hulse
Dr. Anjana Hulse is a seasoned paediatrician in Bangalore with over 15 years of expertise in paediatric endocrine conditions. Her impressive credentials include an MBBS from Rajiv Gandhi University, an MRCPCH from London, and an MSc in Paediatric Endocrinology from the University of Glasgow. Specializing in diabetes, growth disorders, and childhood obesity, Dr. Hulse is dedicated to providing holistic and personalized care. With a track record of treating over 25,000+ young patients, she is passionate about enhancing children's health by tackling hormonal issues and encouraging healthy growth.

Dr. Anjana Hulse's Areas of expertise
- General Paediatrics
- Vaccination and Immunization
- Growth disorders (short stature, tall stature)
- Early or delayed puberty
- Type 1 and Type 2 diabetes in children
- Childhood obesity and related hormonal issues
- Thyroid disorders (hypothyroidism, hyperthyroidism)
- Adrenal gland disorders
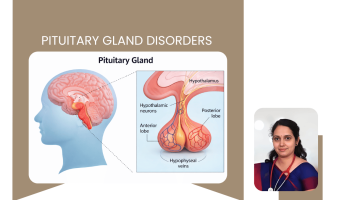
- Pituitary gland disorders
- Metabolic bone diseases (including rickets)
- Polycystic Ovary Syndrome (PCOS) in adolescents
- Menstrual irregularities in teenage girls
- Hormonal imbalances in children and adolescents
- General paediatric endocrinology consultation and follow-up
Article on Precocious puberty:
https://www.happiesthealth.com/articles/parenting/preventing-early-puberty-gnrh-analogues
- MBBS, Rajiv Gandhi University of Health Sciences, Bangalore, India (2002)
- MRCPCH (Membership of the Royal College of Paediatrics and Child Health), UK (2007)
- MSc in Paediatric Endocrinology (Clinical), University of Glasgow & Royal Hospital for Sick Children, Glasgow (2009) – passed with distinction
- Paediatric training placements at premier UK institutions: General Infirmary at Leeds and Royal Hospital for Sick Children, Glasgow
- Fellowship exposure at Sick Kids’ Hospital, Toronto, Canada specializing in metabolic bone disorders and type 1 diabetes in children
This solid academic and clinical foundation in paediatric endocrinology forms the backbone of Dr. Hulse’s expertise in treating complex childhood hormonal and growth-related conditions.
Book Appointment
Hulse Clinic 635, 8th Main Rd, Jeewan Griha Colony, phase 2, J. P. Nagar, Bengaluru, Karnataka 560078
Clinic Hours:
- Monday - Friday
- 10:30 AM - 01:00 PM 06:00 PM - 09:00 PM
Contact:
Phone: 9480260001
Email: [email protected]
Conditions and Treatments









Dr. Anjana Hulse's Expert Tips & Health Insights
Articles by Dr. Anjana Hulse
By:
Dr. Anjana Hulse
10 June 2025
Understanding Childhood Obesity and When to Seek Help
One of the more sensitive concerns parents bring to my clinic is weight gain in children. "She’s always been chubby, but now she’s gaining too fast.
Read More
By:
Dr. Anjana Hulse
10 June 2025
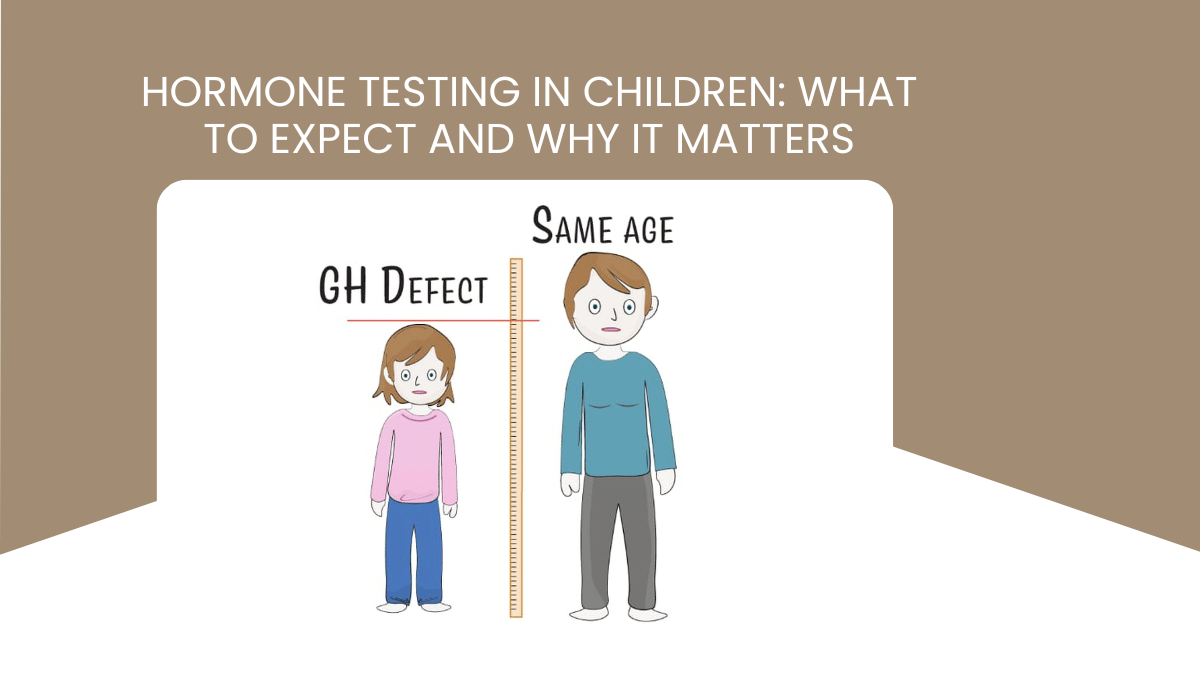
Hormone Testing in Children: What to Expect and Why It Matters
As a paediatric endocrinologist, I often meet parents who are worried about their child’s growth, early or delayed puberty, sudden weight gain, or unexplained fatigue.
Read More
By:
Dr. Anjana Hulse
10 June 2025
Is Your Child Growing Normally What Parents Should Know About Growth Disorders
One of the most common questions I hear from parents is, “Is my child growing normally?” As a pediatric endocrinologist, I understand how important and sometimes stressful it can be for parents to monitor their child’s height and weight.
Read More
By:
Dr. Anjana Hulse
10 June 2025
Understanding Childhood Obesity and When to Seek Help
One of the more sensitive concerns parents bring to my clinic is weight gain in children. "She’s always been chubby, but now she’s gaining too fast.
Read More
By:
Dr. Anjana Hulse
10 June 2025
Hormone Testing in Children: What to Expect and Why It Matters
As a paediatric endocrinologist, I often meet parents who are worried about their child’s growth, early or delayed puberty, sudden weight gain, or unexplained fatigue.
Read More
By:
Dr. Anjana Hulse
10 June 2025
Is Your Child Growing Normally What Parents Should Know About Growth Disorders
One of the most common questions I hear from parents is, “Is my child growing normally?” As a pediatric endocrinologist, I understand how important and sometimes stressful it can be for parents to monitor their child’s height and weight.
Read More
Dr. Anjana Hulse's Reviews
Sort By:
Dr. Anjana Hulse's Reviews
Frequently Asked Questions
Sort By:
Frequently Asked Questions
Share
Yes! AI models are being developed to predict a child’s future height and to improve personalized insulin dosing—though data privacy and validation remain challenges.
Share
Bone age helps assess growth by comparing skeletal maturity to chronological age. Significant misalignment can indicate hormone disorders and guide treatment timing.
Share
Puberty blockers (GnRH agonists) can delay early puberty in children with precocious puberty.
Share
If they show rapid height changes, weight issues without clear cause, early puberty signs, body odor in young children, or constant thirst/urination—these warrant specialist evaluation.
Share
Precocious puberty: under 8 (girls) or under 9 (boys) with signs like breast development or testicular enlargement. Delayed: no signs by age 13 in girls or 14 in boys.
Share
Consider timing, underlying causes, genetic growth potential, side‑effects (rare headaches or hip issues), and long‑term monitoring of growth and bone health.
Share
GH therapy is considered for children with hormone deficiencies or idiopathic short stature. Start early—before puberty—for best outcomes. It requires stimulation tests and thorough consultation.
Share
Common tests include hemoglobin A1C, C‑peptide, ketones, and diabetes-related antibodies—particularly if there’s a family history.
Share
There’s no fixed screening age, but experts suggest testing kids around ages 2, and again between 5–7, especially if symptoms like extreme thirst, frequent urination, weight loss, hunger, fatigue, or irritability appear.
Share
Link copied to clipboard!